

Translate this page into:
A Systematic Review of Vestibular Evoked Myogenic Potential in Individuals with Motion Sickness
Address for correspondence Krishna Yerraguntla, PhD, CCC-A, Department of Speech and Hearing, Manipal College of Health Professions (MCHP), Manipal Academy of Higher Education (MAHE), Manipal, Karnataka, 576104, India (e-mail: krishna.y@manipal.edu).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The otolith of vestibular system in the human body helps in maintaining the static balance. Travelling can cause defect in static balance that may lead to motion sickness. The evidence showing the relation between vestibular evoked myogenic potential (VEMP) that assesses otolith function and motion sickness is contrasting. The current systematic review is aimed to understand outcomes of published articles in reporting association between vestibular evoked myogenic in individuals with motion sickness. For this study, the database used is PubMed, Scopus, ProQuest, CINHAL, and Web of Science. The data is extracted from the final articles where VEMP is done on individuals with and without motion sickness. The total articles included are 125 out of which five articles used for the systematic review. In this study, motion sickness susceptibility questionnaire is used to assess individuals with and without motion sickness. The latency and amplitude of both cervical VEMP (cVEMP) and ocular (oVEMP) of individuals with and without motion sickness are normal. However, the review indicates a significant change in the interaural asymmetry ratio of both cVEMP and oVEMP results in individuals with motion sickness. This shows that there might be a variation in the functional asymmetry in the otoliths. From the review, it is clear that there might be otolith changes due to motion sickness that can have a smaller impact on the interaural asymmetry ratio in VEMP. These findings can be further applied for the diagnostic purpose in individuals with motion sickness.
Keywords
cervical vestibular evoked myogenic potentials
motion sickness
ocular vestibular evoked myogenic potentials
otolith organ

Introduction
The inner ear is divided into an auditory and vestibular system where the auditory system is responsible for hearing, whereas the vestibular system is for balance and spatial alertness. The semicircular canals and the otolith organs of the vestibular system give equal inputs for maintaining the equilibrium. Two otolithic structures, utricle and saccule, contain hair cells and supporting cells within the macula. The otoconia present inside the utricle and saccule keep up the inertia when there is an increase in the outside gravity.1
The balance system is controlled by multisensory input from the visual, spatial, and vestibular systems. This system consists of several reflex actions that are essential for its functioning. The most relevant reflexes in this system are the vestibulo-spinal reflex and the vestibulo-ocular reflex. When there is a sudden sense of posture variation in the surroundings, the hair cells and otoconia in the utricle and saccule along with the semicircular canal trigger an ocular and spinal reflex to maintain the balance. The utricle is for horizontal and saccule is for vertical static balance. When there is horizontal and vertical motion, the hair cells of the utricle and saccule tends to move in the opposite direction of the movement and there will be an inability to focus on a particular image. This is because of the depolarization that happens from the movement of the hair cells that will be sent to the brain for maintaining balance.2 If there is a disarray of vestibular, visual, and proprioception, that will give the sense of central nervous confusion and as a defense it initiates vomiting.3
Similar is the case of motion sickness. According to Dennison and D’Zmura,4 the possibility of motion sickness occurs when the brain's incoming sensory input is mismatched to the actual signals obtained. It is generally seen when the compensatory mechanism of vestibular ocular reflex is lagged by 10 ms creating confusion within the brain.5 This confusion can cause dizziness, nausea, cold sweating, and salivation. This kind of mismatch in the system is seen in each individual and varies according to each person's susceptibility and stimulus intensity. It was believed that motion sickness had major contributions from the visual system, causing alterations in the vestibular system. However, later it was found that even a blind person could develop motion sickness.6 This shows that it is not the visual system, but that the vestibular system plays a major role in motion sickness susceptibility.
In order to assess the vestibular system, the most commonly used test is vestibular evoked myogenic potential (VEMP). VEMP is of short latency and is recorded by presenting high-intensity acoustic stimuli. The vestibular system initiates the VEMP response and gives precise ear-specific information about the otolith nerve function and the reflexes.7 The tests, ocular vestibular evoked myogenic potential (oVEMP) and cervical vestibular evoked myogenic potential (cVEMP), are used to evaluate vestibulo-ocular and vestibulo-spinal reflexes, respectively. VEMP findings are interpreted by analyzing the P1 and N1 peak latencies, amplitudes as well as the interaural asymmetry ratio (IAAR).
Studies have shown that VEMP can be utilized to identify susceptibility to motion sickness.8,9 There is evidence that the amplitude asymmetry ratios between the VEMP results of people vulnerable to motion sickness are distinct from normal. This is because when there is an accelerated force given to the head, the heavier part of otoconia is tilted. In motion sickness individuals, the latency to get the position of the membrane to its initial matrix gets increased and thus results in asymmetry. Also, the density of the membrane plays an important role in causing this asymmetry.10 Larger asymmetries among ocular reflex for right and left side incline are found to be vulnerable to motion sickness.11
There are also contrasting evidence on the relation between VEMP and motion sickness. The research done by Boldingh et al12 showed that VEMP on individuals with vestibular migraine and motion sickness found latency was more affected in individuals having migraine and motion sickness rather than individuals with just motion sickness. Hence, there is a necessity to understand if the otolith organ is affected because of motion sickness. Additionally, there is a need to understand the association between VEMP and motion sickness reported in the literature. This systematic review is done to understand the association of VEMP results on motion sickness individuals published to date.
Methodology
This systematic review was conducted to understand outcomes of published articles in reporting an association between the VEMP in individuals with motion sickness. Approval for the current study was obtained from Institutional Research Committee (IRC) (Appendix A1) and PROSPERO registration (CRD42021240581) (Appendix A2).
Data Source
The current systematic review study on VEMP and motion sickness was carried out in December 2020. It was published on the PROSPERO register database. The database used for the respective study is PubMed, Scopus, ProQuest, CINHAL, and Web of Science. The key terms used for the study are (“Motion sickness” AND “Vestibular evoked myogenic potential”), (“Motion sickness” AND “VEMP”), (“Motion sickness” AND “Occular Vestibular evoked myogenic potential”), (“Motion sickness” AND “oVEMP”), (“Motion sickness” AND “cervical Vestibular evoked myogenic potential”), (“Motion sickness” AND “cVEMP”), (“Motion sickness” AND “ Electrophysiological tests”), (“Motion sickness” AND “Vestibular Function”).
Eligibility Criteria
The articles were included based on the inclusion and exclusion criteria.
Inclusion criteria:
Articles published between January 2010 to December 2020
Original research
Research dedicated to motion sickness while travelling through the road where they have used VEMP to study balance issues
Exclusion Criteria
Literature review, editorials
Full text not available
Study designs other than case-control and cohort studies
Articles not published in English
The articles were found by using an assortment of key terms. The different database was downloaded and was imported to the Rayyan software. The duplicate articles were then removed in the software itself. The rest of the selected articles were assessed by the independent reviewers. The conflict articles were then reviewed by the third reviewer. The articles were excluded if the research was done using different vestibular tests other than VEMP or if the articles were done on altered motion sickness like seasickness, space sickness, and cybersickness. Studies done on animal populations were eliminated along with studies that do not include the required key terms.
Data Extraction
The demographic data such as the age and gender of the participants were noted. The hearing evaluation tests and results showed the presence of any abnormality of the ear. These tests include pure tone audiometry and tympanometry. The consumption of any drugs or alcohol before the testing was determined. Motion sickness susceptibility questionnaire (MSSQ) was used to draw out motion sickness in the population. This test material consists of three sections to check the duration, type, and severity of the individuals. The VEMP results participants with and without motion sickness were taken separately. The amplitude and latency of P1N1 and N1P1 were taken out along with interaural amplitude, latencies, and IAAR. The calculation was done using statistical analysis in each study.
Article Quality Assessment
The risk of bias of the different articles was determined using the Downs and Black checklist13 for clinical trial quality assessment. The subtests of the checklist include reporting, external validity, internal validity, internal validity confounding (selection bias), and power. Two questions were considered not applicable and were subtracted from the total score of 32. The proportion of 30 in low, moderate, and high-quality scaling is considered on a unit of 10. Where 0 to 10 is considered low quality, 10 to 20 is moderate quality, and above 20 is high quality. Therefore, all the articles are high quality.
Results
The final number of studies received was 125 out of which 29 were duplicates. After the analysis from the independent reviewers, the conflict articles were eight and were resolved by the third independent reviewer. The final included articles after excluding the studies by eliminating criteria were five (►Fig. 1).
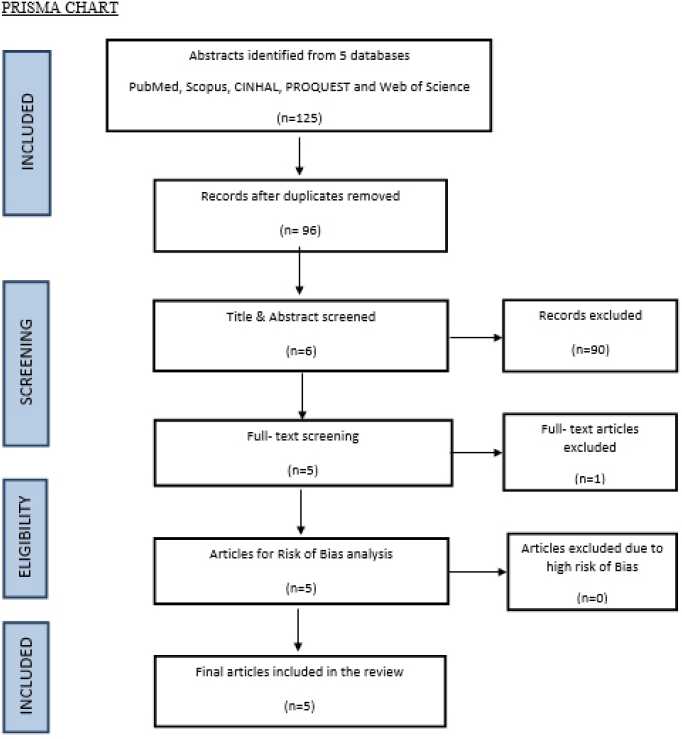
- PRISMA flow diagram
Motion Sickness
All the five studies included were case-control studies. The participants in the experimental group and control group were divided into equal numbers ranging from around 20 to 30 individuals, respectively. Participant's ages ranged between 17 and 40 years in all five studies. MSSQ determined the severity of motion sickness. A study done by Buyuklu et al14 showed 90% of people having carsickness, 70% of seasickness, 30% elevator sickness, and 10% had air sickness. Nausea and drowsiness are common symptoms that were seen in all the motion sickness susceptible participants. They found women tend to be more susceptible than men. The research done by Fowler et al15 showed that eight participants showed high severity, seven showed mild/ moderate, and the remaining showed low severity in MSSQ with nausea being a consistent symptom of the individuals. Xie et al16 used MSSQ for 54 participants where 23 people showed susceptibility to motion sickness. All the susceptible individuals had symptoms of nausea and drowsiness. Sixteen people had vomiting. Eighty-five percent of people showed carsickness. Singh et al17 considered 90 individuals for the study, where 30 participants showed high severity in carsickness. The rest 60 people taken were normal and for professional drivers, the motion susceptibility was found to be low. In the study, by Neupane et al,18 participants having high susceptibility scores were included. Thirty individuals showed susceptibility to motion sickness.
Vestibular Evoked Myogenic Potential
See ►Table 1.
| References | Buyuklu et al14 2009 | Xie et al16 2012 | Fowler et al15 2014 | Singh et al17 2014 | Neupane et al18 2018 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Country | Turkey | China | Mexico | India | India | ||||
| No. of participants with MS | 20 | 26 | 24 | 30 | 30 | ||||
| Gender | M/F | 11/9 | 26 M | 5/19 | NA | NA | |||
| Age in years (mean) | 26 | 21.5 | 23 | 29 | 21 | ||||
| Acoustic stimuli | cVEMP | RE | S | P1 (ms) | 16.29 ± 1.75 | 14.3 ± 3.3 | 13.59 ± 1.22 | ||
| N1 (ms) | 25.49 ± 2.13 | 20.02 ± 2.3 | 20.55 ± 1.79 | ||||||
| NS | P1 (ms) | 16.02 ± 1.3 | 14.6 ± 1.5 | 13.25 ± 0.96 | |||||
| N1 (ms) | 25.37 ± 1.95 | 20.09 ± 1.4 | 20.77 ± 1.39 | ||||||
| LE | S | P1 (ms) | 14.32 ± 5.05 | 14.1 ± 2.4 | 13.78 ± 1.32 | ||||
| N1 (ms) | 22.65 ± 8.03 | 20.4 ± 2.1 | 20.97 ± 1.53 | ||||||
| NS | P1 (ms) | 15.94 ± 1.49 | 15.0 ± 1.7 | 13.06 ± 1.02 | |||||
| N1 (ms) | 25.13 ± 1.3 | 20.8±4.2 | 20.79 ± 1.34 | ||||||
| Combined RE+ LE | S | P1 (ms) | 15.43 | ||||||
| N1 (ms) | 24.81 | ||||||||
| NS | P1 (ms) | 15.49 | |||||||
| N1 (ms) | 25.07 | ||||||||
| IAAR S/NS | Latency | 8.66/9.32 | 6.0/6.8 | 34.56/17.60 | |||||
| Amplitude | 86.38/70.5 | 82.8/57.61 | 9.12/21.11 | 66.58/78.56 | |||||
| S/NS | Threshold (dBnHL) | 61.05/78.31 | |||||||
| oVEMP | RE | S | N1 (ms) | 10.36 ± 0.68 | |||||
| P1 (ms) | 15.24 ± 1.2 | ||||||||
| NS | N1 (ms) | 10.35 ± 0.74 | |||||||
| P1 (ms) | 15.11 ± 0.87 | ||||||||
| LE | S | N1 (ms) | 10.74 ± 0.61 | ||||||
| P1 (ms) | 15.21 ± 0.95 | ||||||||
| NS | N1 (ms) | 10.63 ± 0.73 | |||||||
| P1 (ms) | 15.28 ± 1.10 | ||||||||
| Combined RE+ LE | S | N1 (ms) | 11.5 | ||||||
| P1 (ms) | 15.84 | ||||||||
| NS | N1 (ms) | 11.24 | |||||||
| P1 (ms) | 16.23 | ||||||||
| IAAR S/NS | Latency | 4.79/4.75 | |||||||
| Amplitude | 13.47/13.1 | 7.85/16.4 | |||||||
| S/NS | Threshold (dBnHL) | 85.14/89.53 | |||||||
Abbreviations: MS, motion sickness; cVEMP, cervical vestibular evoked myogenic potential; IAAR, interaural asymmetry ratio; LE, left ear; NS, nonsusceptible individual; oVEMP, ocular vestibular evoked myogenic potential; RE, right ear; S, susceptible individual.
Discussion
Motion Sickness Susceptibility
Motion sickness is a natural occurrence that nearly everyone would experience at some stage in their lives. Low-frequency vertical, horizontal, angular, rotary, or simulated simulator motion to which a person has not adapted could lead to motion sickness. There were mainly five articles used for the systematic review. The articles reviewed in the study consist of individual's ages ranging from 17 to 40 years. The relation of gender is mentioned only in one study where it showed motion sickness susceptibility is seen common in women than in men.14 MSSQ was used to assess individuals with and without motion sickness in the studies. The majority of studies with individuals having motion sickness exhibited common symptoms such as vomiting, drowsiness, salivation, cold sweating, and nausea. In all the studies, the participants had motion sickness susceptibility and had high risk and history of sickness and they were having symptoms at least for the past 10 years. According to the MSSQ diagnosis, the individuals were more exposed to roadways. Hence, they exhibited more carsickness (90%) than seasickness (70%). The study by Buyuklu et al14 and Xie et al16 mentioned that all the motion sickness susceptible individuals showed the presence of nausea and drowsiness more than other symptoms. Fowler et al,15 Singh et al,17 and Neupane et al18 separated motion sickness individuals with normal using the MSSQ short questionnaire. It divided the individuals based on the severity. The participants were divided based on severity because the more severe individual showed a better correlation to the findings than normal. The division based on types of motion sickness helped to understand what type of balancing system is involved in these cases. In most of the studies, heterogenous motion sickness is considered. In the case of carsickness, the visual and vestibular system plays a key role rather than in seasickness where all the three somatosensory, visual, and vestibular systems have an equal part.
Vestibular Evoked Myogenic Potential
Physiological studies on the vestibular system such as VEMP have been inconclusive in determining the effect of the motion sickness. The latency and amplitude of both cVEMP and oVEMP of individuals with and without motion sickness were usually compared in those studies.
cVEMP and Motion Sickness
In all the studies used in the systematic review, P1N1 latencies of cVEMP were observed and compared between the experimental group and control group. The latencies of P1N1 were within the normal range. An individual with motion sickness can develop a compensatory strategy for balance. This can elicit normal values in cVEMP latencies. Four out of five studies are done on the correlation of cVEMP and motion sickness. The studies done by Buyuklu et al,14 Singh et al,17 and Neupane et al18 had no significant difference with normal. This could be due to less sample size taken by the authors or because of the large standard deviation. Buyuklu et al14 did not assess the physical activity of the participants. This may be a factor leading to subclinical vestibular findings. The study by Fowler et al15 found higher amplitude in the susceptible individuals than nonsusceptible individuals. The reason mentioned was that the participants who were very sensitive to motion sickness can have hyperactive reflexes. Hyperactivity of the reflexes can cause higher deviation in the cVEMP amplitudes. Since cVEMP assesses the vertical motion of the body, when there is a change in vertical motion, the amplitudes can be higher. However, the remaining studies did not show any significant findings in amplitude.
oVEMP and Motion Sickness
There are two studies done to analyze the relation between oVEMP and motion sickness susceptibility. The N1P1 latencies and amplitude of these studies showed no correlation between the susceptible and nonsusceptible individuals. According to Xie et al,16 there could be a compensatory mechanism involved when the balance of the human body is affected. Hence, the neural impulses are observed to be intact.
Threshold Estimation
The study by Singh et al17 was the only study where the threshold of both cVEMP and oVEMP was observed. With a decrease in the stimulus intensity, they were able to find elevated results in the threshold of the susceptible and nonsusceptible groups. The poor threshold found in motion sickness susceptibility individuals implied reduced functioning of otolith organs.
Interaural Asymmetry Ratio
Two of three studies17,18 found an association with IAAR of amplitudes in motion sickness susceptible individuals. The IAAR of both cVEMP and oVEMP in Singh et al17 and Neupane et al18 was found to be reduced in the experimental group. Some susceptible individuals had smaller amplitude in the left and some in the right ear. Motion sickness does not have ear specificity for diagnosis. In one study done by Xie et al,16 it is mentioned that if their study had additional samples the asymmetry ratio would have been present, since they had a large standard deviation in the IAAR of the amplitude of motion sickness individuals. Neupane et al18 reported that the reason for asymmetry is that when the two otoliths send an unequal quantity of impulses to the brain, the dilemma in the cortical region causes intoxication. These intoxications are then reversed by reflexes of the body such as nausea, dizziness, or vomiting.
In the current review, amplitudes and latencies of both cVEMP and oVEMP were normal. But there is a significant change in the IAAR of both cVEMP and oVEMP results in most of the studies. This shows that there might be a variation in the functional symmetry in the otoliths, because of sensory conflict in space and due to weight variability that is seen in them. From this, it can be derived that there might be otolith changes due to motion sickness. This systematic review is done as an exploratory attempt to understand the association between VEMP and individuals who are susceptible to motion sickness. Further studies are needed to confirm the relation.
Conclusion
This systematic review was done to understand the association of VEMP results on individuals susceptible to motion sickness. Out of the 125 articles taken, only five articles were included in the study. A significant change was seen in the IAAR compared to amplitude and latency in individuals susceptible to motion sickness. From the review, it is clear that there might be otolith changes due to motion sickness that can have a smaller impact on the VEMP. These findings can be further applied for the diagnostic purpose in individuals with motion sickness.
Conflict of Interest
None declared.
References
- Anatomy of the vestibular system: a review. NeuroRehabilitation. 2013;32(3):437-443.
- [CrossRef] [PubMed] [Google Scholar]
- Vestibular system: anatomy, physiology, and clinical evaluation. In: Somatosensory and Motor Research. Intech Open 2020 doi:10.5772/intechopen.90538
- [CrossRef] [Google Scholar]
- Motion sickness: an evolutionary hypothesis. Science. 1977;197(4302):493-495.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of unexpected visual motion on postural sway and motion sickness. Appl Ergon. 2018;71:9-16.
- [CrossRef] [PubMed] [Google Scholar]
- Handbook of Virtual Environments: Design, Implementation, and Applications. Lawrence Erlbaum Associates 2002:773-790.
- [Google Scholar]
- Male and female characteristics in vestibular testing: a step toward the selection of the best participants for space flight. Acta Astronaut. 1980;7(11):1323-1331.
- [CrossRef] [PubMed] [Google Scholar]
- Stanney KM, ed. Handbook of Virtual Environments: Design, Implementation, and Applications. Lawrence Erlbaum Associates 2002:773-790.
- [Google Scholar]
- Seasickness pathogenesis and the otolithic organs: vestibular evoked myogenic potentials study-preliminary results. Isr Med Assoc J. 2007;9(9):641-644.
- [Google Scholar]
- Vestibular evoked myogenic potentials and habituation to seasickness. Clin Neurophysiol. 2013;124(12):2445-2449.
- [CrossRef] [PubMed] [Google Scholar]
- The sense of balance in humans: Structural features of otoconia and their response to linear acceleration. PLoS One. 2017;12(4):e0175769. 10.1371/journal.pone.0175769
- [CrossRef] [PubMed] [Google Scholar]
- The relative roles of the otolith organs and semicircular canals in producing space motion sickness. J Vestib Res. 1998;8(1):57-59.
- [CrossRef] [PubMed] [Google Scholar]
- Vestibular sensitivity in vestibular migraine: VEMPs and motion sickness susceptibility. Cephalalgia. 2011;31(11):1211-1219.
- [CrossRef] [PubMed] [Google Scholar]
- The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384.
- [CrossRef] [PubMed] [Google Scholar]
- Vestibular functions in motion sickness susceptible individuals. Eur Arch Otorhinolaryngol. 2009;266(9):1365-1371.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of motion sickness severity on the vestibular-evoked myogenic potentials. J Am Acad Audiol. 2014;25:814-822.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular vestibular evoked myogenic potentials and motion sickness susceptibility. Aviat Space Environ Med. 2012;83(1):14-18.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of otolith function using cervical and ocular vestibular evoked myogenic potentials in individuals with motion sickness. Ergonomics. 2014;57(12):1907-1918.
- [CrossRef] [PubMed] [Google Scholar]
- Higher asymmetry ratio and refixation saccades in individuals with motion sickness. J Am Acad Audiol. 2018;29(2):175-186.
- [CrossRef] [PubMed] [Google Scholar]




